A new study by a team of scholars, headed by DUPRI's Michelle White and Naomi Duke, examines the factors that protect children from developing obesity despite the presence of risk factors. The paper, currently in press at Academic Pediatrics, is titled "Positive Outliers: A Mixed Methods Study of Resiliency to Childhood Obesity in High-Risk Neighborhoods."
Despite the high prevalence of obesity and the clustering of risk by neighborhood, few studies have examined characteristics which promote healthy child weight in neighborhoods with high obesity risk. The authors aimed to identify protective factors for children living in neighborhoods with high obesity risk.
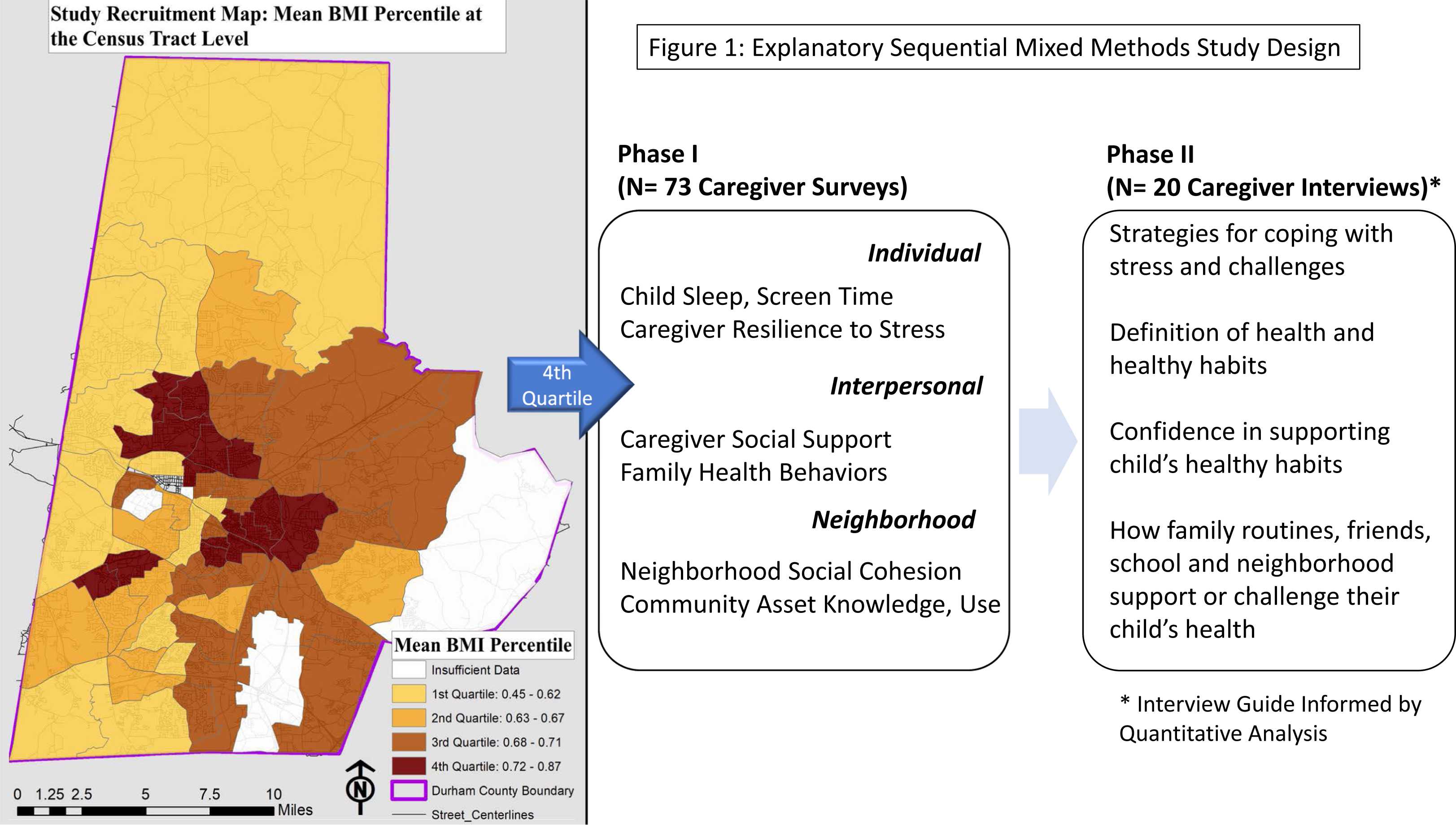
The authors identified neighborhoods with high obesity risk using geolocated electronic health record data with measured body mass index (BMI) from well child visits (2012-2017). They then recruited caregivers with children aged 5-13 years who lived in census tracts with mean child BMI percentile > 72 (February 2020- August 2021). They used sequential mixed methods (quantitative surveys, qualitative interviews) to compare individual, interpersonal and perceived neighborhood factors among families with children at healthy weight (positive outliers, PO) vs. families with ≥1 child with overweight or obesity (controls). Regression models and comparative qualitative analysis were used to identify protective characteristics.
Seventy-three caregivers participated in the quantitative phase (41% PO; 34% preferred Spanish) and twenty in the qualitative phase (50% PO; 50% preferred Spanish). Frequency of healthy caregiver behaviors was associated with being a PO (Family Health Behavior Scale Parent Score adjusted β 3.67; 95% CI 0.52-6.81 and qualitative data). Protective factors also included caregivers’ ability to minimize the negative health influences of family members and adhere to family routines.
There were few differences between PO and control families. Support for caregiver healthy habits and adherence to healthy family routines emerged as opportunities for childhood obesity prevention in neighborhoods with high obesity risk.
In neighborhoods with high risk of child obesity, families with healthy weight children and families with children with overweight/obesity are behaviorally and socially similar. Parental modeling and support for healthy behaviors across children’s environments may promote healthy child weight.
PO were largely similar to control families. Frequency of healthy caregiver behaviors and family members’ support for healthy child behaviors (i.e., behavioral modeling) are potential protective factors. The protective effects of behavioral modeling at the school and neighborhood levels warrants further investigation. These findings point to the importance of child obesity interventions which incorporate multiple health influences including caregivers and extended family.